A review of catecholamine synthesis and a brief introduction to terminologies such as fractionated metanephrines, plasma metanephrines and catecholamines.
Synthesis of Catecholamines
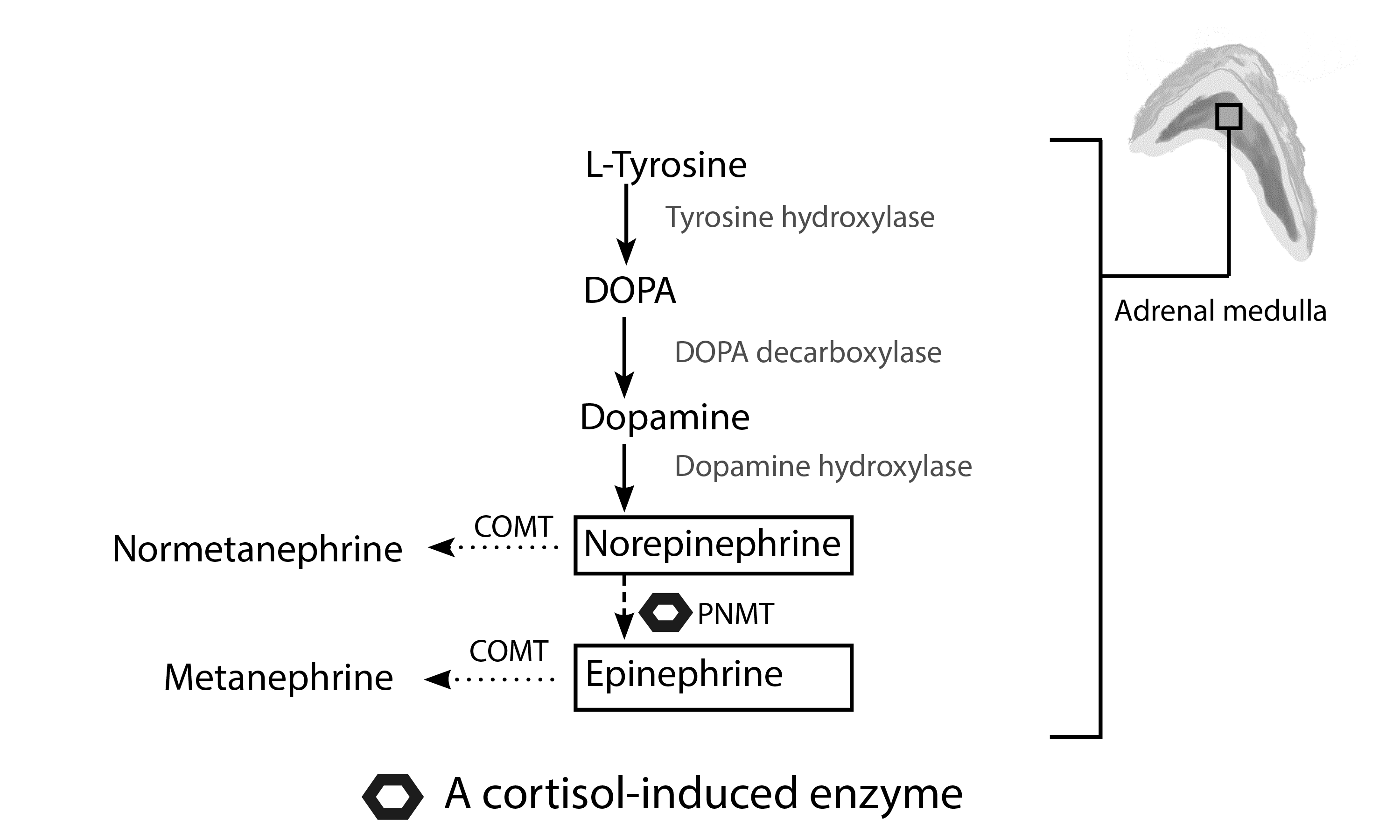
Fig. 1 Schematic diagram of catecholamine synthesis. The rate-limiting step in the synthesis of catecholamine occurs at the initial conversion of L-tyrosine into L-3,4-dihydroxyphenylalanine (DOPA) via the tyrosine hydroxylase enzyme. DOPA is subsequently converted to dopamine. Dopamine is hydroxylated into L-norepinephrine, which is then converted into epinephrine. The conversion of norepinephrine to epinephrine requires the cortisol-induced enzyme, phenylethanolamine-N-methyl transferase (PNMT)(dashed arrow)[1].
This is the reason why epinephrine and its metabolite (metanephrine) are only produced by PNMT-containing organs such as chromaffin cells in the adrenal gland and the organ of Zuckerkandl (located at the aortic bifurcation). Norepinephrine and epinephrine are converted into their metabolites, i.e., normetanephrine and metanephrine, respectively, by catechol-O-methyltransferase (COMT)(dotted arrow)[2]. (Based on Grouzmann et al. (2015) Catecholamine Metabolism in Paraganglioma and Pheochromocytoma: Similar Tumors in Different Sites? PLOS ONE 10:e0125426)
Cortisol and PNMTCortisol stimulates phenylethanolamine-N-methyl transferase (PNMT).
Catecholamines and fractionated metanephrines (Understanding terminology)
- Continuous intratumoral conversion of catecholamines (epinephrine and norepinephrine) into their metabolites (metanephrine and normetanephrine respectively) by COMT, makes fractionated metanephrines either in plasma or urine a valuable screening tool. Catecholamines are, however, released intermittently, as such, screening tests involving the use of only catecholamines might miss a PPGL[3].
- The term fractionated metanephrines refers to the metabolites of epinephrine and norepinephrine; these are metanephrine and normetanephrine, respectively[4].
- Clinically significant elevation of epinephrine or metanephrine (its metabolite) almost always implies the presence of adrenal PNMT, a cortisol-induced enzyme, although present in extra-adrenal tissues like paraganglia, is not under paracrine stimulation by cortisol in these tissues and, therefore, does not convert norepinephrine into epinephrine[5].
Clinical Pearl
What is the pathophysiologic basis of hypotension in patients in pheochromocytomas?
Hypotension is usually an unexpected finding in patients with pheochromocytoma. Clinicians should, however, be aware of the possibility of a paradoxical decrease in blood pressure in patients with PPGLs[6]. Interestingly there are even reports of hypotension and hypertension rarely co-existing in rapid cycling paroxysms[7].
Pathophysiology
- Prolonged activation of adrenergic receptors causes profound arterial and venous vasoconstriction. This process results in a reduction in cardiac output (hypotension), which is sensed by baroreceptors, leading to a compensatory increase in catecholamine release. This catecholamine surge causes sustained hypertension, which invariably activates the baroreceptor reflex arc again, leading to hypotension[8].
- Sustained hyperstimulation of catecholamine receptors promotes their downregulation, following which there is hypotension during periods of low catecholamine secretion[9, 10].
References
- Zuber SM, Kantorovich V, Pacak K (2011) Hypertension in Pheochromocytoma: Characteristics and Treatment. Endocrinol Metab Clin North Am 40:295–311
- Grouzmann E, Tschopp O, Triponez F, et al (2015) Catecholamine Metabolism in Paraganglioma and Pheochromocytoma: Similar Tumors in Different Sites? PLOS ONE 10:e0125426
- Grouzmann E, Drouard-Troalen L, Baudin E, Plouin P-F, Muller B, Grand D, Buclin T (2010) Diagnostic accuracy of free and total metanephrines in plasma and fractionated metanephrines in urine of patients with pheochromocytoma. Eur J Endocrinol 162:951–960
- Kim HJ, Lee JI, Cho YY, et al (2015) Diagnostic accuracy of plasma free metanephrines in a seated position compared with 24-hour urinary metanephrines in the investigation of pheochromocytoma. Endocr J 62:243–250
- Kantorovich V, Pacak K (2010) Pheochromocytoma and paraganglioma. Prog Brain Res 182:343–373
- Mabulac MP, Abad LR (2013) Pheochromocytoma presenting as hypotension in a 12 year old female. Int J Pediatr Endocrinol 2013:P117
- Ionescu CN, Sakharova OV, Harwood MD, Caracciolo EA, Schoenfeld MH, Donohue TJ (2008) Cyclic Rapid Fluctuation of Hypertension and Hypotension in Pheochromocytoma. The Journal of Clinical Hypertension 10:936–940
- Kobal SL, Paran E, Jamali A, Mizrahi S, Siegel RJ, Leor J (2008) Pheochromocytoma: cyclic attacks of hypertension alternating with hypotension. Nature Reviews Cardiology 5:53–57
- Shin E, Ko KS, Rhee BD, Han J, Kim N (2014) Different effects of prolonged β-adrenergic stimulation on heart and cerebral artery. Integr Med Res 3:204–210
- Kassim TA, Clarke DD, Mai VQ, Clyde PW, MohamedShakir KM (2008) Catecholamine-Induced Cardiomyopathy. Endocrine Practice; Jacksonville 14:1137–1149