

Introduction
Thyroid nodules (TN) are discrete lesions within the thyroid gland, detectable by palpation or visualized using imaging techniques such as ultrasound. TNs are among the most common endocrine disorders, with palpable nodules observed in approximately 4-7% of the general population. However, these figures considerably underestimate their prevalence, as high-resolution ultrasound (US) reveals their presence in almost every adult. Despite the commonality of TN, less than 1% possess malignant potential. However, given its potentially life-threatening implications, an accurate and efficient evaluation process is crucial.
Diagnostic evaluation of Nodular Thyroid Disease
TSH Determination
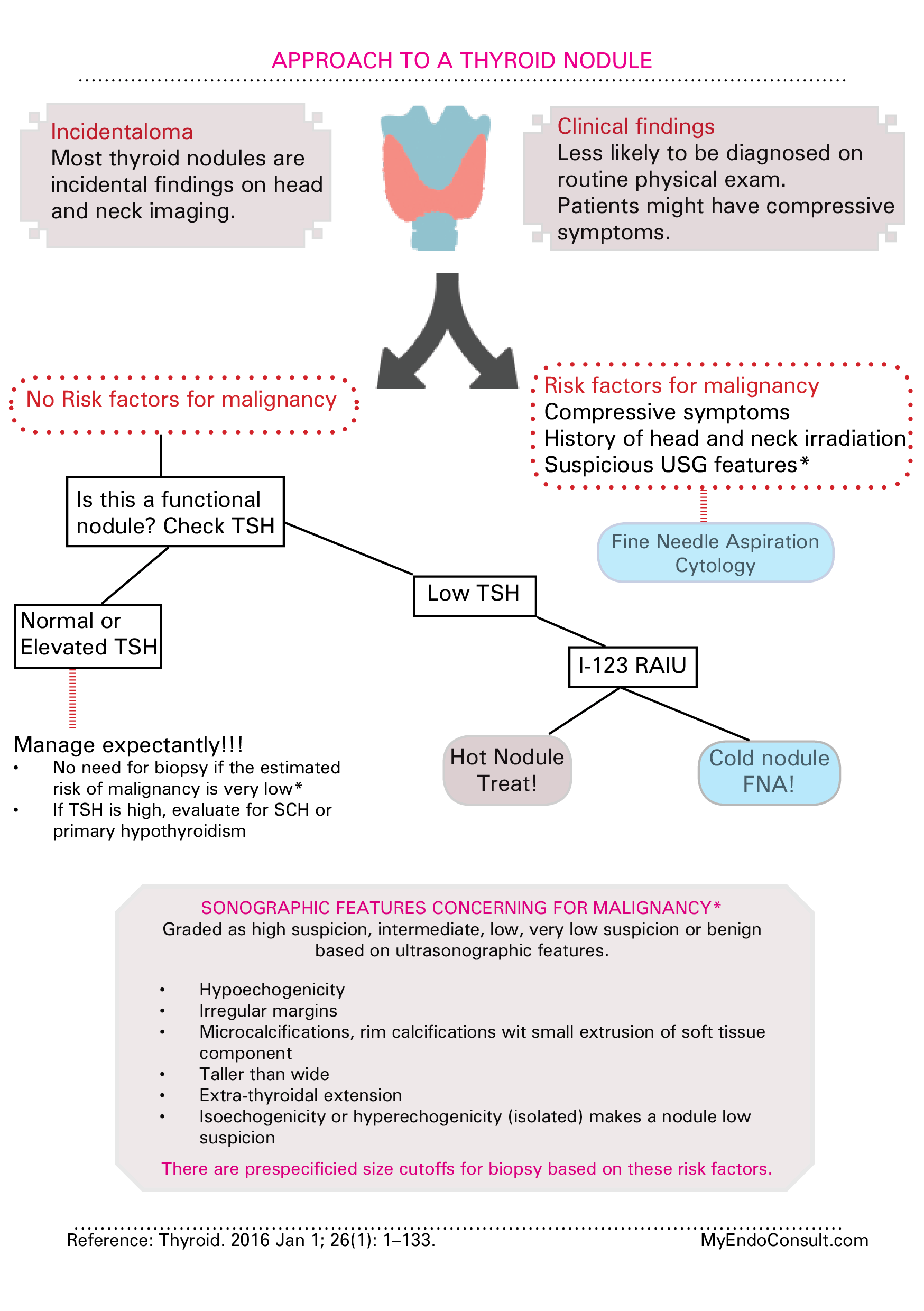
A serum thyroid stimulating hormone (TSH) test is generally the first step in assessing TN. Lower than normal TSH levels might indicate hyperfunction of the nodules and warrant further assessment using a radionuclide thyroid scan. However, normal or elevated TSH levels require the use of ultrasound-guided fine needle aspiration (FNA) for diagnostic clarification.
Ultrasound Imaging
Thyroid ultrasound is a crucial tool in TN evaluation due to its non-invasive nature, accessibility, and ability to provide detailed images of the structure of the thyroid gland. It helps characterize the nodules’ size, number, location and specific features, such as composition (solid, cystic, or mixed), echogenicity, shape, margin, and presence of calcifications or abnormal lymph nodes.
Although ultrasound is a sensitive tool, it is operator dependent. Therefore, the skill and experience of the individual performing and interpreting the scan significantly influence its diagnostic value.
Fine needle aspiration
The Thyroid Imaging Reporting and Data System (TIRADS) is a classification system that is used in the evaluation and reporting of thyroid ultrasound findings. The goal of the TIRADS classification is to help predict the risk of malignancy in thyroid nodules, thus helping in clinical decision-making regarding the need for biopsy or monitoring.
The classification of TIRADS is based on the ultrasound characteristics of the thyroid nodules, including their composition (solid, cystic, or mixed), echogenicity (hyperechoic, isoechoic, hypoechoic, or very hypoechoic), shape (wider than tall or taller than wide), margin (smooth, irregular, or poorly defined) and presence or absence of echogenic foci.
There are several different versions of the TIRADS classification, including the American College of Radiology (ACR) TIRADS, the European Thyroid Imaging Reporting and Data System (EU-TIRADS) and the Korean Thyroid Imaging Reporting and Data System (K-TIRADS).
These systems vary in their specifics, but all aim to standardize the interpretation of thyroid ultrasound findings and improve the accuracy of risk stratification for thyroid nodules. The use of these classification systems has been shown to reduce the number of unnecessary thyroid biopsies while still effectively identifying nodules that are likely to be malignant.
The Bethesda System for Reporting Thyroid Cytopathology
Fine needle aspiration (FNA) is a critical tool for the evaluation and management of thyroid nodules. The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) was established in 2008 to standardize the interpretation and reporting of FNA results. This system classifies thyroid FNA results into six categories, each with an implied risk of malignancy and recommended management approach.
Bethesda I: Nondiagnostic or Unsatisfactory
Species in this category are inadequate for diagnosis due to limited cellularity, obscuring blood or clotting, or poor preservation. The risk of malignancy ranges from 1 to 4%, and the typical recommendation is to repeat the FNA.
Bethesda II: Benign
This category includes benign follicular nodules, colloid nodules, thyroiditis, or other benign entities. The implied risk of malignancy is low (<1%), and the usual management approach is clinical follow-up without immediate surgical intervention.
Bethesda III: Atypia of unknown significance or Follicular lesion of Undetermined Significance (AUS/FLUS)
This category is used for samples that exhibit atypical cellular or architectural characteristics that cannot be definitively classified as benign or malignant. The risk of malignancy ranges from 5-15% and recommended management can involve repeat FNA or molecular tests, depending on the patient’s clinical scenario.
Bethesda IV: Follicular Neoplasm or Suspicious for Follicular Neoplasm
This category is reserved for samples suggesting a follicular neoplasm. The risk of malignancy is approximately 15-30%. Diagnostic surgical excision, often a lobectomy, is usually recommended, given the inability of FNA to distinguish between benign follicular adenoma and malignant follicular carcinoma.
Bethesda V: Suspicious of malignancy.
Species in this category have cytological features suggestive but not definitive for malignancy. This category has a risk of malignancy of 50-75%, and is generally recommended to perform a near-total or total thyroidectomy.
Bethesda VI: Malignant
This category is used for specimens with cytological features consistent with malignancy, including papillary thyroid carcinoma, medullary thyroid carcinoma, undifferentiated (anaplastic) carcinoma, or lymphoma. The risk of malignancy is nearly 97-99% and a near-total or total thyroidectomy is usually recommended, depending on the subtype of cancer and the overall health status.
Genomic Classifier Studies for Suspicious Thyroid Nodules: Insights from ThyroSeq and Afirma
Treatment of thyroid nodules, particularly those that produce indeterminate fine-needle aspiration (FNA) results, presents a clinical conundrum. In recent years, genomic classifier tools such as ThyroSeq and Afirma have emerged as promising adjuncts to guide management decisions. These tools provide genetic analysis of thyroid nodules to stratify the risk of malignancy better.
ThyroSeq is a comprehensive genomic classifier that uses next-generation sequencing to detect genetic alterations associated with thyroid cancer in FNA samples. It examines a broad range of genetic markers, including point mutations, gene fusions, copy number alterations, and gene expression alterations.
ThyroSeq has been shown to have high sensitivity and specificity to rule out and rule out malignancy in thyroid nodules, reducing the need for diagnostic surgery in many cases. The ThyroSeq test can classify most indeterminate nodules (Bethesda III, IV, V) as the high or low risk of cancer, helping clinicians make decisions about surgery versus surveillance.
Afirma is another genomic sequencing classifier that is used in the evaluation of thyroid nodules. It uses microarray technology to analyze the expression of genes associated with thyroid malignancy, creating a gene expression classifier (GEC).
Afirma is typically used when FNA cytology results are indeterminate. A ‘benign’ Afirma result has been shown to correlate with a benign histopathological result strongly, thus reducing the need for surgery in many patients with indeterminate cytology.
The Afirma test has been updated to the Genomic Sequencing Classifier (GSC) and Xpression Atlas (XA), providing additional genomic alteration data and offering improved performance over the original GEC.
Nodule Management
The treatment of the nodule depends on whether surgical intervention is required or whether non-surgical treatments are sufficient. Traditionally, surgery was the primary approach, but recent advances have introduced effective non-surgical alternatives.
Surgery
Surgical removal of the thyroid gland (thyroidectomy) is a common treatment for large symptomatic nodules, those that harbor cancer or exhibit suspicious characteristics on FNA, and those that cause hyperthyroidism that does not respond to conservative treatments. The extent of surgery (total or partial thyroidectomy) depends on the characteristics and overall health status of the patient.
Nonsurgical Approaches
Non-surgical methods include watching for small, asymptomatic benign nodules and treatments such as radioactive iodine therapy or alcohol ablation for hyperfunctioning nodules. Recently, thermal ablation techniques such as radiofrequency, laser, and high-intensity focused ultrasound ablation have emerged as minimally invasive alternatives to the management of benign thyroid nodules.
Conclusion
Evaluation of thyroid nodules is a multifaceted process that requires a combination of clinical, biochemical, and imaging investigations to determine the appropriate treatment approach. Despite the widespread prevalence of TN, most do not present a health risk. However, efficient diagnostic protocols are essential to identify the small percentage of cancers that can harbor malignancy, ensuring prompt and effective treatment. Further advancements in diagnostic techniques and management strategies will continue to refine our approach to thyroid nodules.
Kindly Let Us Know If This Was helpful? Thank You!