
Adrenal Vein Sampling (AVS)
Interpretation Calculator
Enter the aldosterone and cortisol values from each adrenal vein and from the inferior vena cava (IVC). Indicate whether cosyntropin (ACTH) stimulation was used. Then click Submit.
Disclaimer: This calculator is for informational purposes only. Clinical decisions should be based on a full evaluation and professional judgment.
What is adrenal vein sampling?
The accuracy of computed tomography in diagnosing the source of hyperaldosteronism is poor (about 50%). Adrenal vein sampling (AVS) is thus critical in localizing the source of hyperaldosteronism in patients who opt for surgical amelioration of their disease. However, the results of AVS are operator-dependent and best done in high-volume centers with expertise in performing the test under optimal conditions. Indeed in expert hands, technical success exceeds 90%.
History of adrenal vein sampling
AVS was first proposed and shown to be a reliable diagnostic test in localizing the source of hyperaldosteronism in the 1960s by James Melby and colleagues at the Boston University School of Medicine. They recognized the importance of improving pre-operative diagnostic certainty in cases of ambiguity.
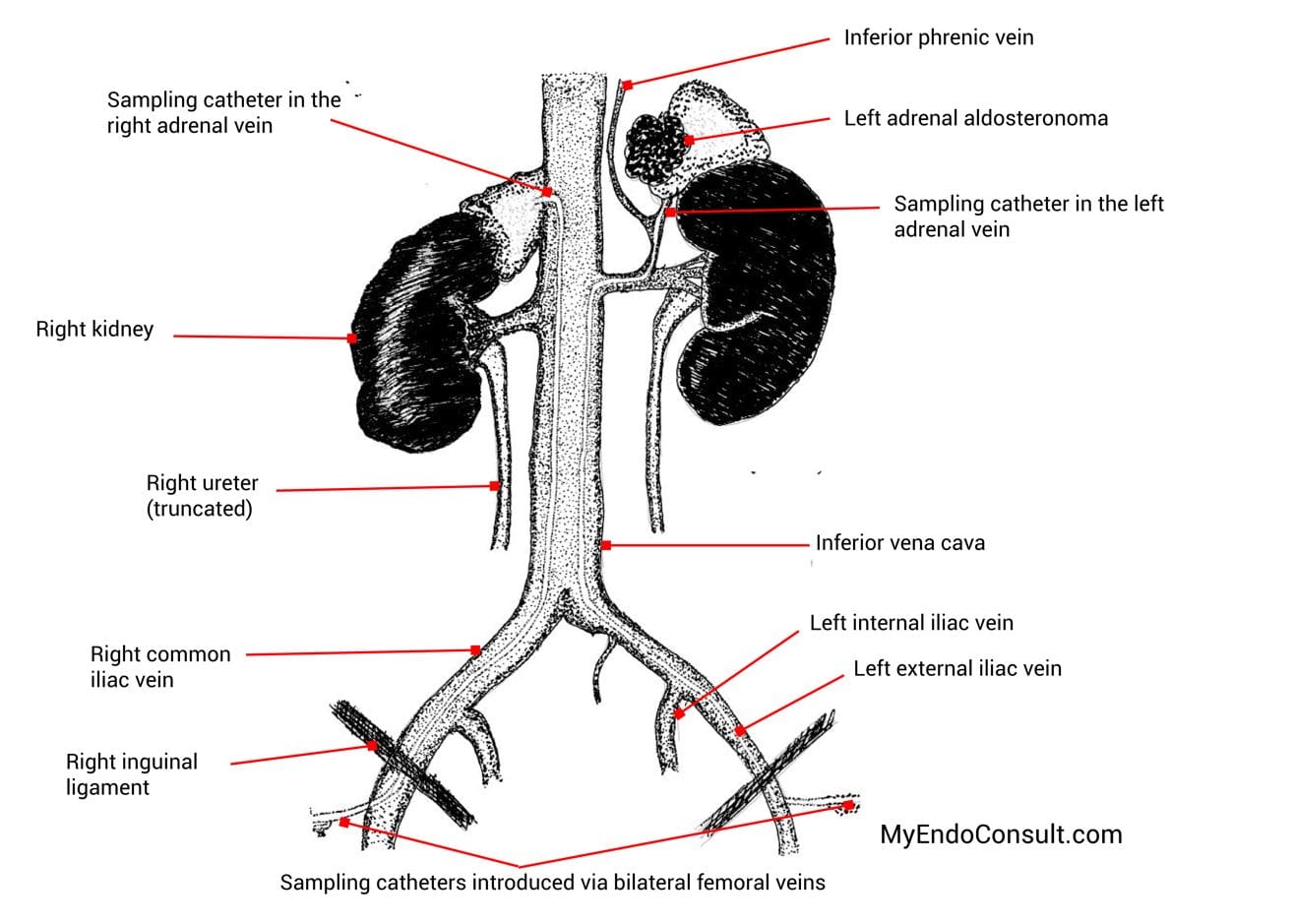
Figure 1. Relevant anatomy of the adrenal gland and venous blood supply.
The right adrenal vein drains directly into the inferior vena cava posteriorly but well above the right adrenal vein. The right adrenal vein can be difficult to cannulate for various reasons including its short course, small caliber size, and rare anomalous source (may arise in conjunction with branches of the hepatic vein). The left adrenal vein abuts off the common inferior phrenic vein. Unlike the right adrenal vein, the left adrenal vein is generally easier to catheterize. The inferior vena cava sample is traditionally obtained from the external iliac vein.
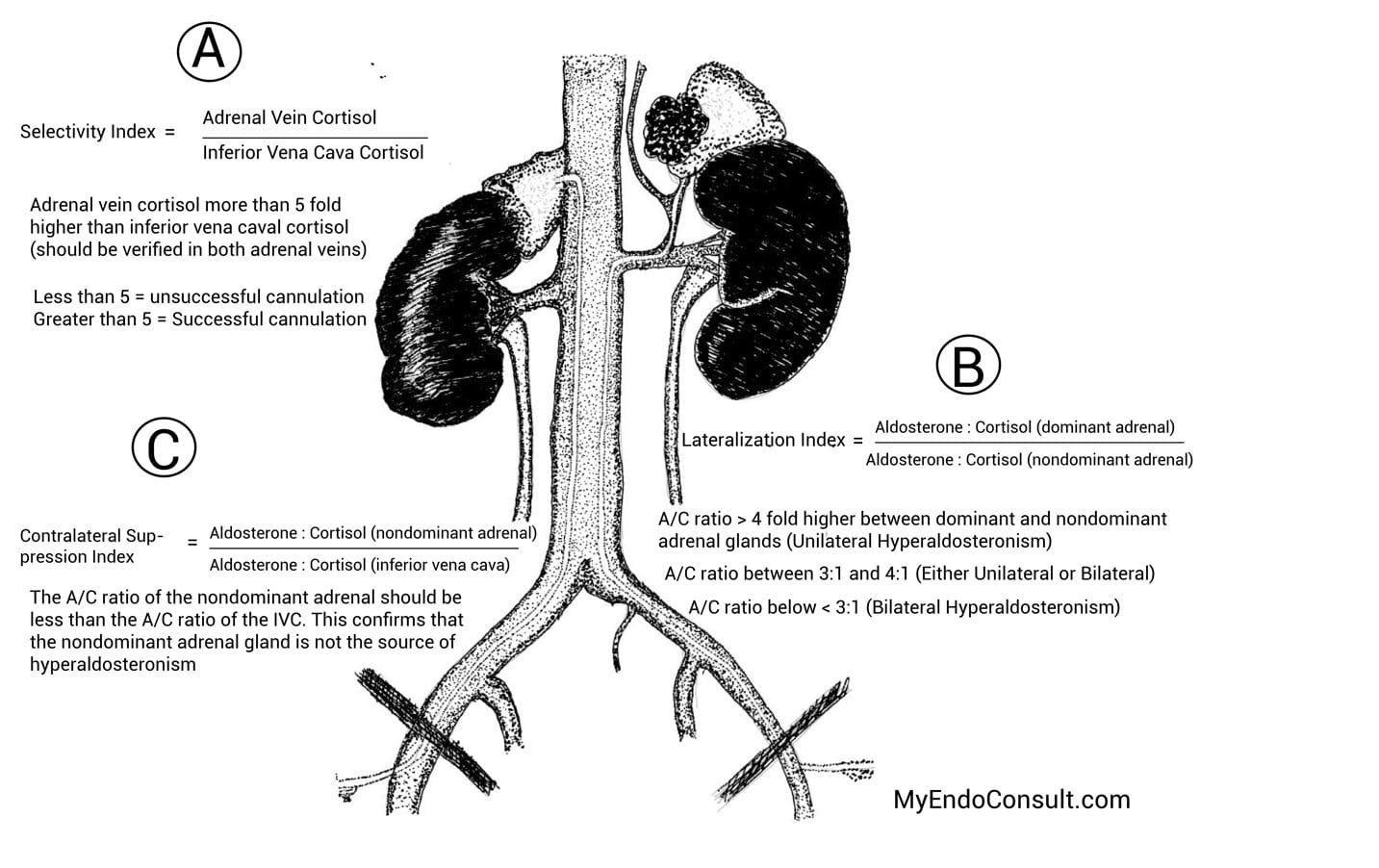
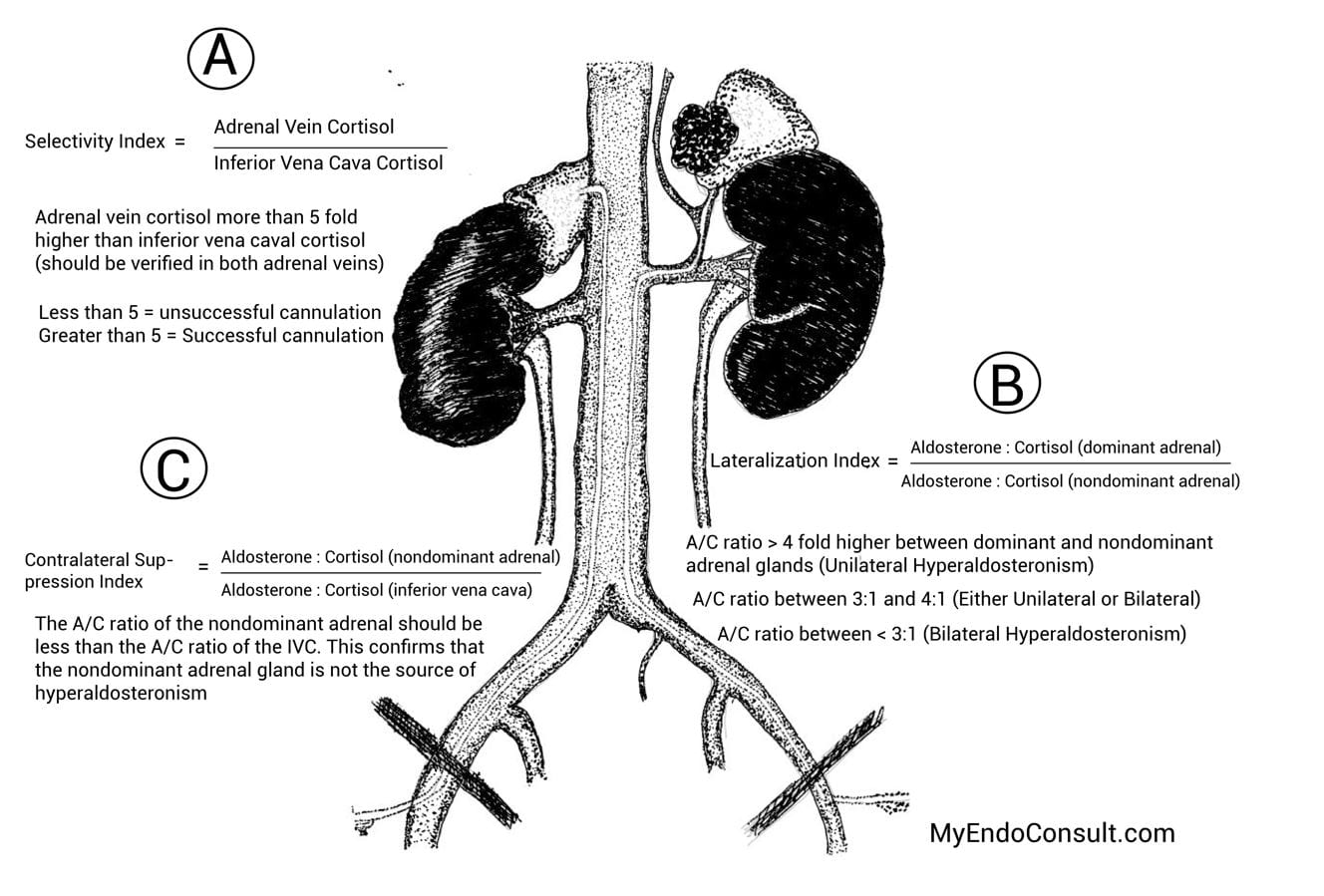
Figure 2. A simplified approach to interpreting adrenal vein sampling
Sequential cannulation of both adrenal veins occurs through a percutaneous bilateral femoral approach under fluoroscopic guidance. Either a 5 or 6 French vascular catheter is placed in the femoral vein, which facilitates the passage of 4 and 5 French catheters into each adrenal vein. The optimal location of the catheter tip is confirmed via contrast enhancement. To reduce the lag time between samples, the right adrenal vein (the most difficult) is sampled first, followed by the left adrenal vein, and finally from the external iliac vein. Aldosterone and cortisol levels are drawn from each site.
Continuous infusion of cosyntropin (at 50mcg per hour) for at least 30 minutes before sampling of the adrenal glands and indeed is maintained for the duration of the procedure. This mitigates stress-induced elevation in aldosterone production. In addition, cosyntropin maximizes the gradient in cortisol (comparing the adrenal gland to the inferior vena cava). Finally, cosyntropin maximizes the output of aldosterone from the source of hyperaldosteronism (be it an aldosterone-producing adenoma or adrenal hyperplasia).
What are the complications of AVS?
- Adrenal hemorrhage
- Adrenal vein dissection
- Groin hematoma (femoral vein)
Optimal Approach to interpreting AVS on the board exam and in clinical practice
Selectivity index
Cortisol level in each adrenal vein is compared to peripheral cortisol in the IVC. The selectivity index (see figure 2, label A) is a ratio of cortisol in the adrenal vein compared to cortisol in the IVC. Although various cutoffs have been proposed, a ratio above 5 on each side is highly suggestive of successful cannulation on each side.
Lateralization index
After successful confirmation of optimal cannulation of both adrenal veins, the next step involves ascertaining the source of excess aldosterone production. The lateralization index (see figure 2, label B). The aldosterone to cortisol levels on each side is determined (A : C ratios for the left and right adrenal veins). The side with the higher A: C ratio (dominant adrenal) is divided by the side with a lower A: C ratio (nondominant adrenal). If the lateralization index is greater than or equal to 4, this is compatible with a unilateral source of hyperaldosteronism involving the side with the higher A: C ratio.
A lateralization index between 4:1 and 3:1 may be either unilateral or bilateral disease. This is inconclusive, and ancillary testing may be required. The involvement of an expert in hyperaldosteronism is needed.
A lateralization index below 3:1 is indicative of bilateral disease. Surgery should therefore be deferred in favor of medical therapy.
Contralateral gland suppression index
The contralateral suppression index is an additional required confirmatory step in cases where there is clear lateralization to a culprit adrenal gland. The aldosterone to cortisol ratio of the nondominant adrenal gland (unaffected side) should either be lower (or equal) to the peripheral A : C ratio
Practice Question
Interpret this adrenal venous sampling (AVS) report and recommend the next step in this patient’s management
| Vein | Aldosterone (A), ng/dL | Cortisol (C), mcg/dL | A : C ratio | Aldosterone Ratio ** |
|---|---|---|---|---|
| Right Adrenal Vein | 9200 | 470 | 19.6 | 65.3 |
| Left Adrenal Vein | 125 | 410 | 0.3 | |
| Inferior Vena Cava | 33 | 10 | 3.3 |
** Right adrenal vein A/C ratio divided by the left adrenal vein A/C ratio. This should always be a ratio of the dominant to nondominant side.
- Perform a left adrenalectomy
- Perform a right adrenalectomy
- Perform bilateral adrenalectomy
- Start Spironolactone
- Incomplete testing, repeat adrenal vein sampling
Step A: Calculate the selectivity index
The cortisol level in each adrenal vein is more than 5 fold higher than the cortisol in the inferior vena cava.
Step B: Calculate the lateralization index
The A : C ratio of the dominant (right adrenal, 19.6) to nondominant (left adrenal, 0.3) adrenal gland is 65.3. The estimated LI is greater than 4. This is diagnostic for a unilateral source of hyperaldosteronism (from the right adrenal gland).
Step C: Calculate the contralateral suppression index
Evaluation of the contralateral suppression index is required in this patient with a unilateral source of hyperaldosteronism. The A : C ratio in the nondominant adrenal (left adrenal vein, 0.30) is less than the A : C ratio in the periphery (inferior vena cava, 3.3).
This implies the left adrenal gland is not the source of hyperaldosteronemia and confirms the right adrenal gland as the source. The correct answer is B (perform a right adrenalectomy)
Review other questions in the adrenal gland quiz (login required)
Selected References
- Melby JC, Spark RF, Dale SL, Egdahl RH, Kahn PC. Diagnosis and localization of aldosterone-producing adenomas by adrenal-vein catheterization. N Engl J Med. 1967 Nov 16;277(20):1050-6.
- Young WF, Stanson AW, Thompson GB, Grant CS, Farley DR, van Heerden JA. Role for adrenal venous sampling in primary aldosteronism. Surgery. 2004 Dec;136(6):1227-35.
Kindly Let Us Know If This Was helpful? Thank You!